
When documents become check boxes
Let me start this by saying, I am all for efficiency, streamlined approaches, and removing unneeded fluff (yes, I get the irony that I said that three times).
But as the behavioral health industry has shifted to a quantity-over-quality mindset, we have lost the meaning behind the five major clinical documents:
The Intake / Biopsychosocial (BPS) Assessment
The Treatment Plan
Ongoing Assessments
The Progress Note
The Discharge Summary
This post will primarily focus on the intake.
Let’s start by reviewing what your state or accrediting bodies might say about this document:
Be done in X number of hours or days from intake.
Ask about X topics (Discharge planning, goals, presenting problem, diagnosis, etc.).
Be signed by a person with X qualifications.
Often, documents are built to meet these exact specifications. When an audit happens, your assessment is praised. You have all the categories, headers, and requirements. Clinicians are trained to fill in the boxes, write their review, meet the timeline, and pump out more with less.
The "letter" of the document is complete.
The Fallout
Let’s look at what happens next in clinics operating this way.
Clawbacks. Misdiagnosis. Inappropriate levels of care. Missed problems. Poorly made treatment plans. AMAs. Client satisfaction reports plummet because they feel like cattle in a chute. Staff burnout skyrockets, requiring even more assessments to maintain census due to the high exit rate. Money is desperately poured into "client engagement activities," and good employees are put on Performance Improvement Plans (PIPs) due to client turnover.
We look at a leaky pipe and think, “Napkins are only $5, and the pipe would cost $500 to repair.” The easy math is to buy the $5 napkins (or worse, label the leaky pipe as a "client-appreciation water feature").
The Real Purpose of the Intake
So, let’s look at how to remedy this. What is the actual PURPOSE of an intake assessment?
If a client comes in with the presenting problem of “I’m anxious,” we may only ask questions directly related to an anxiety diagnosis. We slap a GAD label on them, give a billable diagnosis of F41.9 Anxiety disorder, unspecified, make a treatment plan labeled "Anxiety” with objectives like “Use box breathing,” get a high five from our manager for doing it in 30 minutes, and move on.
“Technically,” we fulfilled the letter of the requirements.
But our first interaction sets the stage for all subsequent decisions, assessments, medications, and referrals. I don’t blame clinicians for missing details; the system has trained (and rewarded) them to hit the surface and move on.
Using the true Biopsychosocial model (the spirit of the document) we look at how the symptoms have impacted all areas of their life. Are they having thyroid issues? Does this run in their family? What do their Adverse Childhood Experiences (ACEs) look like? What have they done to self-treat or medicate? Is this impacting their relationships, or are their relationships impacting them? How has their culture and ethnic background shaped their view of mental health?
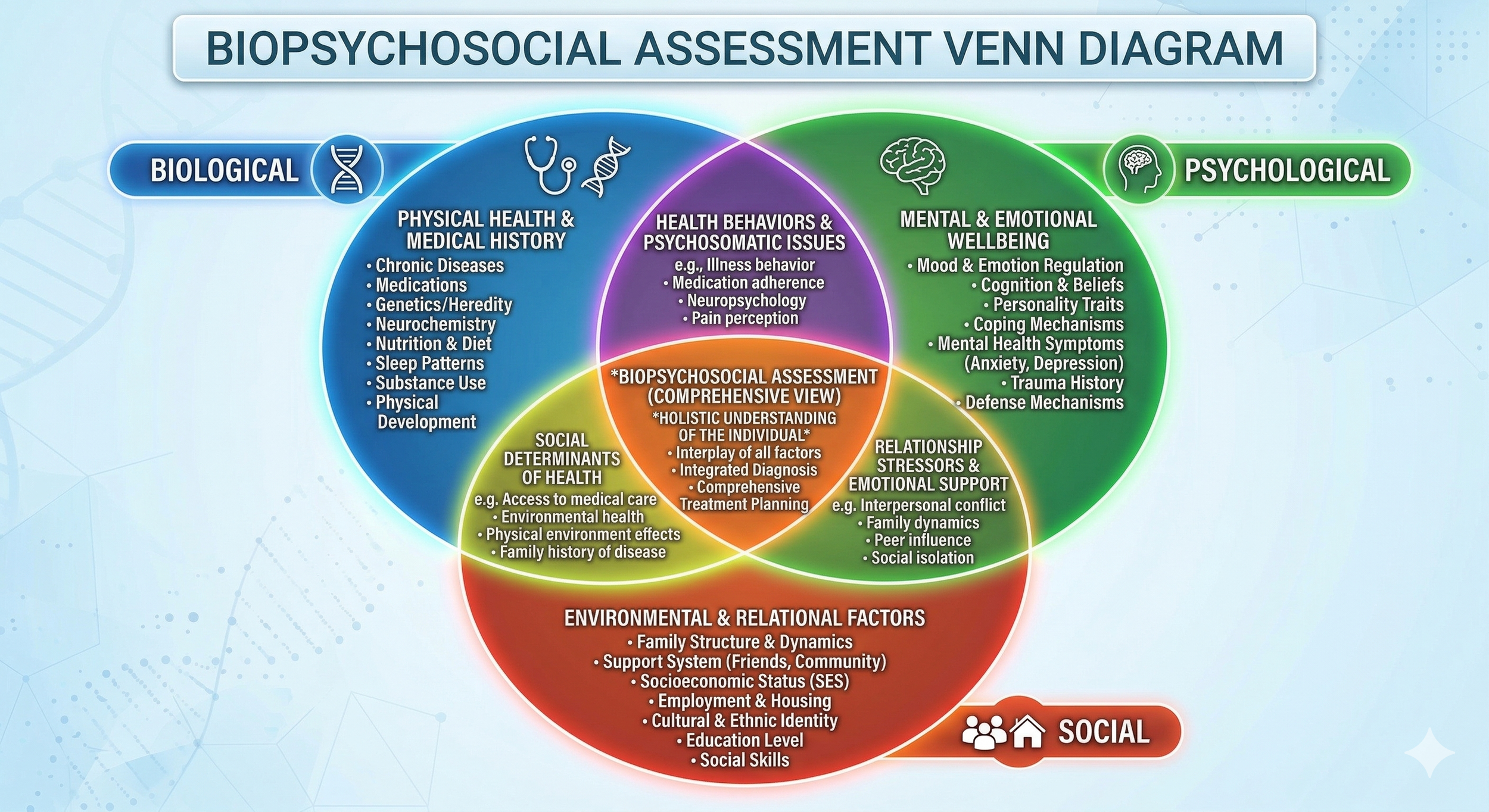
Special thanks to Gemini for producing such a nice diagram.
The Real-World Cost of the Checkbox
To see the clinical and financial risk of sticking to the checkbox, let's look at exactly how that 30-minute "Anxiety" assessment plays out compared to a clinician looking for the "Spirit."
Imagine a 27-year-old client presents to intake reporting: "I worry all the time, I feel tense, and I drink a 6-pack a night to relax." Here is how the exact same interview produces drastically different discoveries depending on how the clinician asks the questions.
The Discovery
Clinician hears "worry" and "drinking" and immediately assumes a generalized Anxiety/Substance presentation.Clinician digs into the function. Client reveals they are late to work because they get stuck in their driveway tapping the steering wheel to prevent a car crash, and drink to paralyze terrifying, intrusive images. The real diagnosis is Obsessive-Compulsive Disorder (OCD).
When we let the checkbox dictate our intake, the output in the chart suffers. The narrative becomes a generic list of symptoms rather than an architectural blueprint of the client's actual life. Notice how the diagnostic validation and problem lists diverge:
Problem Titles
The Checkbox (Surface Level)
Severe Anxiety
Alcohol Abuse
Job Loss
The Clinical Spirit (Deep Formulation)
Intrusive Thoughts & Compulsive Rituals
Chemical Thought-Suppression (Alcohol)
Ritual-Induced Occupational Impairment
Diagnostic Validation
The Checkbox (Surface Level)
Client reports excessive worry and restlessness. Uses alcohol to cope with tension. Meets criteria for GAD and Mild AUD.
The Clinical Spirit (Deep Formulation)
Client exhibits ego-dystonic obsessions (thoughts of harm) and physical compulsions (tapping) consuming >2 hours/day. Alcohol is used functionally to suppress intrusive loops. Meets criteria for OCD.
Ultimately, this dictates the entire trajectory of care. The final clinical summary and treatment recommendations are where the "leaky pipe" either gets fixed or continues to drain your clinic's resources.
Clinical Summary
The Checkbox (Surface Level)
Client presents with persistent worry and sleep issues. Reports recent job loss due to anxiety. Drinks a 6-pack daily to relax. Prognosis is fair with intervention.
The Clinical Spirit (Deep Formulation)
Client presents with severe, intrusive obsessions regarding safety. These obsessions drive time-consuming physical compulsions that directly caused recent job loss. Client utilizes heavy alcohol intake strictly as a neuro-suppressant.
Recommendations
The Checkbox (Surface Level)
Refer to Outpatient Cognitive Behavioral Therapy.
The Clinical Spirit (Deep Formulation)
Refer to specialized Exposure and Response Prevention.
Treatment Plan
The Checkbox (Surface Level)
Goal: Learn deep breathing to reduce tension.
The Clinical Spirit (Deep Formulation)
Goal: Tolerate intrusive thoughts without ritualizing or using alcohol.
The Systemic Impact
When we let the "letter" dictate our intakes, the damage ripples through the entire clinic.
The "Checkbox" client fails out of treatment because deep breathing does not stop OCD compulsions. They drop out AMA, costing the clinic revenue and reinforcing the "leaky pipe" of poor client retention.
The "Spirit" client receives gold-standard ERP therapy, feels truly understood, and naturally drops the alcohol use because the root cause was finally addressed.
Furthermore, by just checking "Uses Alcohol," the clinic misses the severe psychiatric instability underneath, creating a massive safety risk. Conversely, the robust documentation of functional deficits in the deep formulation secures longer insurance authorizations and creates a medical necessity "Golden Thread" that reduces future clawbacks.
Stop Buying Napkins. Fix the Pipe.
An intake document should never just be a list of reasons why a client is sad/anxious; it should be the architectural blueprint for how you are going to help them rebuild their life.
When we let the checkbox dictate our intakes, the damage ripples through the entire clinic. Does this sound familiar? How do your clinic's practices stack up against this reality?
As a compliance and quality assurance consultant, I see this exact leaky pipe draining resources and burning out staff in clinics every single day. The good news? It is entirely fixable. It doesn't require more paperwork; it requires a different lens.
What can I provide to help your team shift their mindset? Whether it is an audit of your current documentation processes, targeted training for your intake clinicians, or a complete structural overhaul of your quality assurance protocols, let's talk.
Stop buying the $5 napkins, and let's actually fix the pipe.
Up Next: The Lost Art of Clinical Interpretation
Wondering where this leaky pipe does the most damage? It’s in the hand-off. In our next post, we are going to tackle the most frequently botched section of the intake: The Clinical Summary. We hire Master's-level clinicians for their expertise, yet our compliance-heavy systems train them to write "book reports" that simply regurgitate the checkboxes above them. We will dive into how training your team to provide true clinical interpretation—rather than just recapping the document—is the only way to rescue your Treatment Plans from becoming just another administrative victim.
Disclaimer: The insights and opinions shared in this post are entirely my own, drawn from my personal experience in the field. They do not represent the views, policies, or operations of my current or past employers. This content is provided for educational and consulting discussions.